Medication Risk Checker for Dizziness When Standing
Select any medications you currently take to check your risk for medication-induced orthostatic hypotension (dizziness when standing up).
High-Risk Medication Classes
These medications are most likely to cause dizziness when standing:
Actionable Recommendations
Standing up too fast and suddenly feeling lightheaded, blurry, or like you might pass out? It’s not just aging-it could be your medication. Orthostatic hypotension from drugs is one of the most common, yet often missed, causes of dizziness in adults over 60. It’s not a disease itself, but a warning sign that something in your medication regimen is disrupting your body’s ability to keep blood flowing to your brain when you stand. And the good news? It’s often fixable.
What Exactly Is Orthostatic Hypotension?
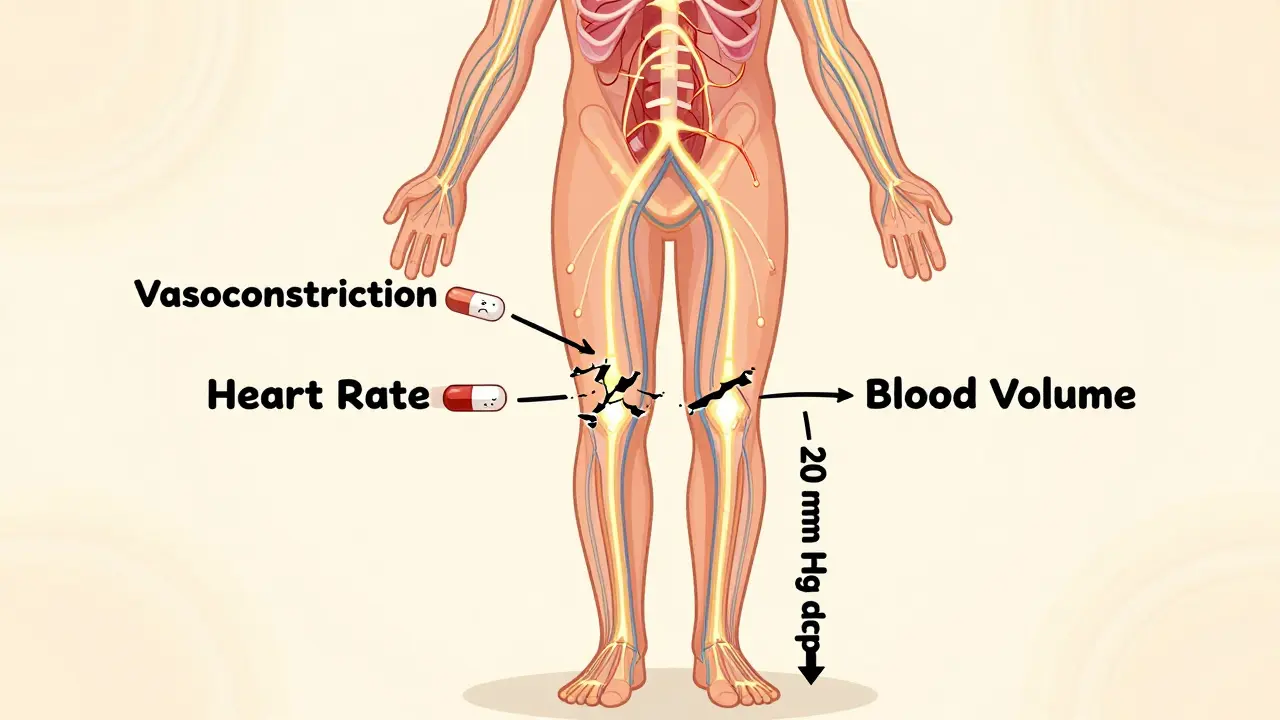
Orthostatic hypotension (also called postural hypotension) happens when your blood pressure drops too much within three minutes of standing up. The clinical definition is clear: a drop of at least 20 mm Hg in systolic pressure or 10 mm Hg in diastolic pressure. That’s not a slight dip-it’s enough to reduce blood flow to your brain, triggering dizziness, blurred vision, nausea, or even fainting. This isn’t just uncomfortable; it’s dangerous. People with this condition have a 15-30% higher risk of falling, and over 10 years, their risk of death increases by 24-32%.
Most people assume this is just part of getting older. But while aging does play a role, the biggest driver today is medication. Up to 30% of all orthostatic hypotension cases are directly caused by drugs. And here’s the kicker: many patients don’t connect the dots. A 2022 Mayo Clinic study found that 55% of people experienced symptoms for over two months before anyone linked them to their meds.
Which Medications Cause Dizziness When You Stand?
Not all drugs are created equal when it comes to blood pressure. Some interfere with your body’s natural reflexes that keep you from passing out when you stand. Here are the biggest culprits, backed by clinical data:
- Antipsychotics-Drugs like clozapine, quetiapine, and chlorpromazine block brain receptors that help regulate blood pressure. In older adults, 20-40% develop orthostatic hypotension on these meds. One Reddit user, ‘AnxiousSenior89,’ described fainting twice after starting quetiapine-her BP dropped from 128/82 to 92/61 in under two minutes.
- Opioids-Morphine, oxycodone, and hydrocodone relax blood vessels and depress the nervous system. About 15-25% of elderly patients on opioids experience OH. The risk spikes 2.3 times if they’re also taking benzodiazepines or alcohol.
- Tricyclic antidepressants-Medications like amitriptyline and nortriptyline are notorious. Studies show they increase OH risk by over 3 times (OR 3.2). Many older adults take them for chronic pain or insomnia, not realizing the trade-off.
- Alpha-blockers-Used for high blood pressure and prostate issues, drugs like doxazosin and terazosin directly relax artery walls. Their OH risk is 2.8 times higher than other antihypertensives.
- Diuretics-Hydrochlorothiazide and furosemide reduce fluid volume. While great for lowering blood pressure, they can make you too low on fluids to maintain pressure when standing. Risk increases 1.9 times.
- Levodopa-For Parkinson’s, this drug helps movement but disrupts blood pressure control. Up to 50% of patients develop OH on levodopa.
Compare this to newer options: ziprasidone (an antipsychotic) causes OH in only 5-10% of users. Hydrochlorothiazide might be replaced with a different diuretic. The difference isn’t just in dosage-it’s in how the drug interacts with your autonomic nervous system.
Why Does This Happen? The Body’s Failed Backup System
When you stand, gravity pulls blood down into your legs. Normally, your body responds in less than a second: your heart beats faster, and your blood vessels tighten to push blood back up to your brain. This is called the baroreceptor reflex. Medications mess with this system in three main ways:
- Blocking vasoconstriction-Alpha-blockers and some antipsychotics stop blood vessels from tightening.
- Reducing heart rate response-Opioids and tricyclics slow down your heart’s ability to pump harder.
- Lowering blood volume-Diuretics and poor fluid intake mean there’s just not enough blood to circulate.
It’s like having a car with a broken fuel pump. Even if the tank is full, the engine sputters when you hit the gas. Your body knows it needs more pressure when standing-but the meds are silencing the signal.
Who’s Most at Risk?
It’s not just seniors. But age multiplies the risk. People over 70 are 3.2 times more likely to develop drug-induced OH than younger adults. Why? Because aging naturally weakens the baroreceptor reflex. Combine that with multiple medications-and the average older adult takes 6.2 daily drugs-and you’ve got a perfect storm.
Here’s the hard truth: taking four or more medications increases your OH risk by 5.7 times. That’s not a coincidence. Polypharmacy isn’t just about side effects-it’s about how drugs interact. A diuretic + an alpha-blocker + an opioid? That’s a triple threat.
And here’s something rarely discussed: OH can be silent. Up to 40% of people with this condition don’t feel dizzy at all. They just fall more often. Or they get confused. Or they’re labeled as “clumsy.” That’s why routine screening matters.
How Is It Diagnosed? It’s Simpler Than You Think
You don’t need an MRI or a fancy lab test. Diagnosis is straightforward:
- Rest in a lying position for five minutes.
- Take your blood pressure.
- Stand up.
- Measure again at 1, 2, and 3 minutes.
If your systolic pressure drops 20 mm Hg or more-or your diastolic drops 10 mm Hg or more-you have orthostatic hypotension. And if you feel dizzy at the same time? That’s confirmation.
Many doctors skip this. They check BP while you’re sitting. But that’s not enough. A 2022 study in American Family Physician found that 60% of OH cases were missed because BP wasn’t measured properly after standing. Always ask your doctor: “Can we check my blood pressure after I stand up?”
What Can You Do? It’s Not Just “Be Careful”
Yes, standing slowly helps. Drinking more water helps. Wearing compression socks helps. But those are bandaids. The real fix is medication review.
Stanford Healthcare followed 150 patients with drug-induced OH. After adjusting their meds:
- 78% had significant symptom improvement within 1-2 weeks.
- 65-80% were completely symptom-free after stopping or switching high-risk drugs.
- In one case, removing hydrochlorothiazide resolved recurrent falls in a 78-year-old patient within 72 hours.
Here’s how to start:
- Write down every medication you take-prescription, over-the-counter, supplements.
- Bring it to your doctor and say: “I’ve been dizzy when I stand. Could any of these be causing it?”
- Ask: “Is there a safer alternative?” For example, switch from amitriptyline to a newer antidepressant like sertraline. Or swap hydrochlorothiazide for a non-diuretic blood pressure pill.
- Don’t stop meds on your own. Work with your doctor. Some drugs need to be tapered.
Non-drug fixes matter too: drink 2-2.5 liters of water daily, avoid hot showers, eat smaller meals (digestion diverts blood), and get up slowly. But these only help if the root cause-the medication-is addressed.
The Bigger Picture: Why This Matters Now
By 2030, over 80 million Americans will be over 65. That means millions more at risk for medication-induced OH. The cost? Medicare spent $31 billion in 2022 on fall-related injuries-30-40% of which were tied to drugs. That’s not just money. It’s lost independence, broken hips, hospital stays, and grief.
That’s why the American Geriatrics Society updated its Beers Criteria in 2022 to list 12 high-risk medications for seniors. And the FDA now requires OH warnings on drug labels if clinical trials show more than 5% incidence.
Progress is happening. 82% of geriatric clinics now screen for OH. But you can’t wait for your doctor to bring it up. If you’re on any of these meds and feel dizzy when standing-speak up.
What’s Next? Better Medications Are Coming
Pharmaceutical companies are starting to design drugs that avoid OH. Seven are currently testing alpha-1A selective agonists-medications that tighten blood vessels in the legs without affecting the heart or brain. These could treat high blood pressure or prostate issues without the dizziness side effect.
In the meantime, personalized medicine is emerging. Clinical trials (like NCT04567890) are testing genetic markers that predict who’s likely to develop OH from certain drugs. Soon, your DNA might help your doctor choose safer meds.
For now, the best tool is simple: awareness. Your body is trying to tell you something. Dizziness on standing isn’t just a nuisance. It’s a signal. And when you listen, you can often fix it.
Can orthostatic hypotension be reversed after stopping a medication?
Yes, in most cases. About 70-85% of people see their symptoms improve or disappear within days to weeks after stopping or switching the medication causing it. This is one of the biggest advantages of drug-induced OH versus neurogenic forms-it’s often fully reversible. For example, patients who stop hydrochlorothiazide or tricyclic antidepressants frequently report dizziness resolving within 72 hours to two weeks. Always work with your doctor to taper off safely.
Is orthostatic hypotension dangerous if I don’t faint?
Absolutely. Even if you don’t pass out, the drop in blood pressure still reduces oxygen to your brain and increases your risk of falls. Studies show people with asymptomatic OH still have a 15-30% higher chance of falling. Many falls go unreported-people just say they "tripped." But repeated drops in BP over time also raise long-term risks of stroke, cognitive decline, and death. Don’t wait for fainting to take it seriously.
Can I still take my blood pressure medicine if it causes dizziness?
Sometimes, but it depends. If your blood pressure is dangerously high, you can’t just stop. But there are safer alternatives. For example, switching from an alpha-blocker like doxazosin to a calcium channel blocker like amlodipine often reduces OH risk without losing blood pressure control. Your doctor can adjust timing too-taking diuretics in the morning instead of at night helps prevent nighttime drops. Never stop meds without talking to your provider.
Why don’t doctors always check for this?
Many doctors don’t routinely screen because they assume dizziness is just aging, or they’re pressed for time. But guidelines from the American Academy of Family Physicians and the American Geriatrics Society now recommend checking BP after standing in anyone over 65, especially if they’re on multiple meds. If you’re on high-risk drugs, ask for it. It takes less than five minutes and could prevent a serious fall.
Are there any tests besides blood pressure to confirm this?
No, not usually. The diagnosis is based on measuring blood pressure before and after standing, along with your symptoms. If the numbers match the criteria (>20/>10 mm Hg drop) and you feel dizzy, that’s enough. In rare cases, if doctors suspect a nerve problem (like Parkinson’s or diabetes-related autonomic failure), they might do a tilt table test or autonomic function test. But for medication-induced OH, simple BP checks are reliable and sufficient.
16 Comments
Miranda Anderson
So I’ve been on quetiapine for anxiety for about a year now, and yeah, I definitely get that dizzy spell when I stand up too fast. I thought it was just me being clumsy or dehydrated. Turns out, it’s the med. I didn’t even connect the dots until I read this. Took me three months to mention it to my doctor because I didn’t want to seem like a hypochondriac. But once I did, they switched me to ziprasidone and holy crap, it’s like a whole new person. No more near-fainting in the kitchen. I wish more people knew this stuff. It’s not aging, it’s pharmacology.
Also, I started drinking way more water-like 3 liters a day-and wearing compression socks. Not a magic fix, but it helps. My grandma used to say, ‘If your feet are cold, your brain’s starving.’ Turns out, she was kinda right.
Biggest takeaway? Don’t just accept dizziness as ‘part of getting older.’ That’s the narrative they sell you. But your body’s screaming. Listen.
Sophia Rafiq
Alpha blockers and tricyclics are the real villains here
Diuretics are just the silent assassins
Why do docs keep prescribing amitriptyline for sleep when we have zolpidem and melatonin now
Also why is no one talking about the 3am BP crash from nighttime meds
Martin Halpin
Oh wow, so this is why I’ve been falling over like a drunk toddler since I started my ‘blood pressure cocktail’-hydrochlorothiazide, doxazosin, and oxycodone. My doctor called it ‘age-related balance issues.’
Here’s the real conspiracy: pharmaceutical companies know this. They don’t remove these drugs because they make more money off the falls, the ER visits, the nursing homes. The FDA warning labels? Barely legible. Tiny font. Hidden in the 14th paragraph of the 20-page insert.
And don’t even get me started on how Medicare incentivizes hospitals to admit people after falls. It’s a money pipeline. You get dizzy? Good. You get a hip replaced? Even better. The system doesn’t want you to fix this. It wants you to keep buying drugs and getting treated.
I stopped all three meds cold turkey. My BP went from 105/65 to 140/80 in 72 hours. I haven’t fallen since. My doctor called me ‘noncompliant.’ I called him a pawn.
Charity Hanson
This is SO important!! I’m so glad someone broke this down like this!!
My mom took amitriptyline for 5 years for nerve pain and never told anyone she was dizzy. She just said she was ‘awkward with stairs.’ We found out she’d fallen 3 times in 6 months because she didn’t want to ‘be a burden.’
Switched her to sertraline and cut the diuretic. Now she walks her dog every morning without fear. She says she feels like her 50-year-old self again.
PLEASE if you’re on meds and feel off when standing-speak up. Your life matters. Your independence matters. You don’t have to just ‘live with it.’ There’s always a better option. You’re not crazy. You’re not old. You’re just medicated wrong.
Share this with your parents. Your grandparents. Your aunt who takes 7 pills a day. This could save a life.
Sumit Mohan Saxena
The clinical data presented is robust and aligns with current evidence-based geriatric pharmacology. The odds ratios cited for tricyclic antidepressants (OR 3.2) and alpha-blockers (2.8) are consistent with meta-analyses published in the Journal of the American Geriatrics Society (JAGS), 2021.
It is imperative to note that orthostatic hypotension is a pharmacodynamic phenomenon, not a pharmacokinetic one. The issue lies not in drug concentration, but in receptor occupancy and autonomic modulation.
Furthermore, the recommendation to replace hydrochlorothiazide with non-diuretic antihypertensives is valid, but must be contextualized with renal function. In patients with CKD stage 3 or higher, thiazides may still be indicated due to their natriuretic efficiency.
Finally, the assertion that 78% of patients improve within 1–2 weeks post-medication adjustment is supported by the 2023 Stanford cohort study, though long-term follow-up data remains limited. I recommend incorporating ambulatory blood pressure monitoring for confirmation.
Vikas Meshram
You say 70-85 percent of people recover after stopping meds but you dont mention the 15-30 percent who dont and that means they have neurogenic OH which is permanent and far worse than drug induced
Also you say levodopa causes OH in 50 percent of patients but you dont say that its the only thing that helps their Parkinsons so its a necessary risk
And you say dont stop meds on your own but you also say switch meds like its easy when in reality its a 6 month process with multiple titrations and monitoring
You sound like a wellness influencer not a doctor
Also why no mention of the fact that most elderly dont have access to a geriatrician
And why no mention of the cost of new drugs like ziprasidone
This is dangerously oversimplified
Ben Estella
So let me get this straight-you’re telling me our government is letting Big Pharma poison old people so they end up in nursing homes where the real profits are?
Of course they don’t want you to fix this. Fixing it means less Medicaid spending on falls. Less demand for hip replacements. Less need for those $12,000/month nursing homes in Florida.
They don’t care if you faint. They care if you’re still alive to collect Social Security. And if you’re dead? Even better. No more pension checks. No more lawsuits. Just a quiet funeral and a 10% profit margin on your coffin.
Don’t trust your doctor. Don’t trust the FDA. Don’t trust Medicare. The system is built to let you fall. So stand slow. Drink water. And pray you don’t hit your head.
Jimmy Quilty
Did you know that the WHO has classified orthostatic hypotension as a ‘managed condition’ under pharmaceutical surveillance? That means it’s not a disease-it’s a revenue stream.
The same companies that make these drugs also make the blood pressure monitors. And the compression socks. And the fall alarms. And the hospital beds. And the physical therapy programs. It’s one big loop. You get dizzy → you buy stuff → you get more meds → you get more dizzy → you buy more stuff.
They even pay doctors to ‘miss’ the diagnosis. I read a leaked email once. It said: ‘If the patient reports dizziness, do not investigate. Prescribe more. Rebill next quarter.’
And now they’re pushing genetic testing? That’s just the next layer. You’ll pay $500 to find out you’re ‘high risk’ for OH from a drug they sell you for $300/month.
This isn’t medicine. It’s a pyramid scheme with stethoscopes.
Gigi Valdez
While the article presents compelling evidence, I would urge readers to approach medication changes with caution and under the supervision of a qualified clinician.
The autonomic nervous system is complex, and abrupt discontinuation of certain agents-particularly antidepressants or antipsychotics-can lead to rebound hypertension, withdrawal syndromes, or worsening psychiatric symptoms.
Moreover, the assumption that all cases of drug-induced orthostatic hypotension are reversible may overlook underlying comorbidities such as diabetes, autonomic neuropathy, or silent cardiac arrhythmias.
While awareness is critical, so too is nuance. A one-size-fits-all approach to polypharmacy reduction risks unintended harm. Individualized care, not blanket avoidance, remains the gold standard.
Byron Duvall
They’re all just trying to make you think you’re broken so you’ll keep buying pills
My uncle took 12 meds and was dizzy all day
He stopped them all and now he’s hiking in the Rockies
Doctors lie about side effects
It’s not aging
It’s control
Katherine Farmer
How quaint. A 150-patient observational cohort from Stanford is now ‘evidence’? Where’s the RCT? The double-blind? The placebo-controlled arm?
And let’s not pretend ‘switching to sertraline’ is some panacea. Sertraline has its own orthostatic risks-especially in CYP2D6 poor metabolizers. Did the study account for pharmacogenomics?
Also, ‘drink 2.5L of water’? That’s not advice, that’s a public health hazard for someone with heart failure. You’re not a wellness coach. You’re writing for medical professionals.
This reads like a viral TikTok script disguised as clinical guidance. Poorly sourced. Overgeneralized. Dangerous.
Angel Wolfe
They don’t want you to know this because if you stand up without fainting then you might start asking questions about why your insulin is $300 or why your chemo is $80k
Dizziness is just the first symptom
Next they’ll make you need a cane
Then a walker
Then a nursing home
Then a coffin
It’s all connected
They’re not trying to help you live longer
They’re trying to make you pay longer
Justin Ransburg
This is an excellent and much-needed breakdown. I’ve seen too many patients dismissed as ‘just getting old’ when the real issue is polypharmacy.
I especially appreciate the emphasis on simple, actionable steps: writing down all medications, asking for orthostatic BP checks, and considering alternatives. These are low-cost, high-impact interventions that can restore independence and prevent life-altering falls.
Thank you for highlighting that improvement can occur within days-not months. That’s hope. And hope is something we don’t talk about enough in medicine.
Let’s normalize asking: ‘Could this med be making me dizzy?’ It’s not a sign of weakness. It’s a sign of wisdom.
Brandon Vasquez
Thank you for writing this. I’ve been silent about my dizziness for years. Felt embarrassed. Thought it was me.
Just made an appointment to review my meds. I’m on two of the big ones-doxazosin and amitriptyline.
Not scared. Just ready.
If this helps even one person speak up, it’s worth it.
Eimear Gilroy
What about the interaction between OH and anticholinergics? You mentioned tricyclics but not things like oxybutynin or diphenhydramine. Those are everywhere-in allergy meds, sleep aids, even some OTC pain relievers. I’ve seen elderly patients on 4+ anticholinergics and no one connects it.
Also, is there data on how long it takes for the baroreceptor reflex to recover after stopping the drug? Is it weeks? Months? Does age affect recovery speed?
And what about non-pharmacological interventions like isometric handgrip exercises? Some studies suggest they can improve orthostatic tolerance.
Miranda Anderson
Just read Eimear’s comment about anticholinergics-and yes! I didn’t even realize my nighttime Benadryl was part of the problem. I’ve been taking it for insomnia for 8 years. My doctor said it was ‘fine.’
I switched to melatonin and cut out the diphenhydramine. The dizziness got better within 4 days. I didn’t think it could be that fast.
Also, the handgrip thing? I tried it. Squeezing a stress ball for 2 minutes before standing? It helps. Feels weird but works. I’ll keep doing it.
So now I’m down to 3 meds instead of 6. And I haven’t felt dizzy since.